Arkansas has remained in the top 15 in the amount of medications collected since the first DEA National Drug Take Back Day event started on Sept. 25, 2010. Though the state is 33rd in population with slightly more than 3 million people, Arkansas ranks 4th nationally in pounds collected per capita and 13th in total weight collected.
To date, more than 187 tons (374,457 pounds) of medications have been collected in Arkansas. Nationally, to date, more than 11,669 tons (23,339,120 pounds) of medications have been collected.
The 18th Drug Take Back Day, held on Oct. 26, 2019, resulted in a total medications collection of 441.5 tons nationally, and 13.8 tons was collected from Arkansas. The state ranked 8th in the amount of law enforcement agencies participating in the semi-annual Drug Take Back Day with 192 agencies and ranked 13th in the number of Drug Take Back Day collection sites with 183 locations (the number doesn’t include the permanent drop box locations where many take back day events were held).
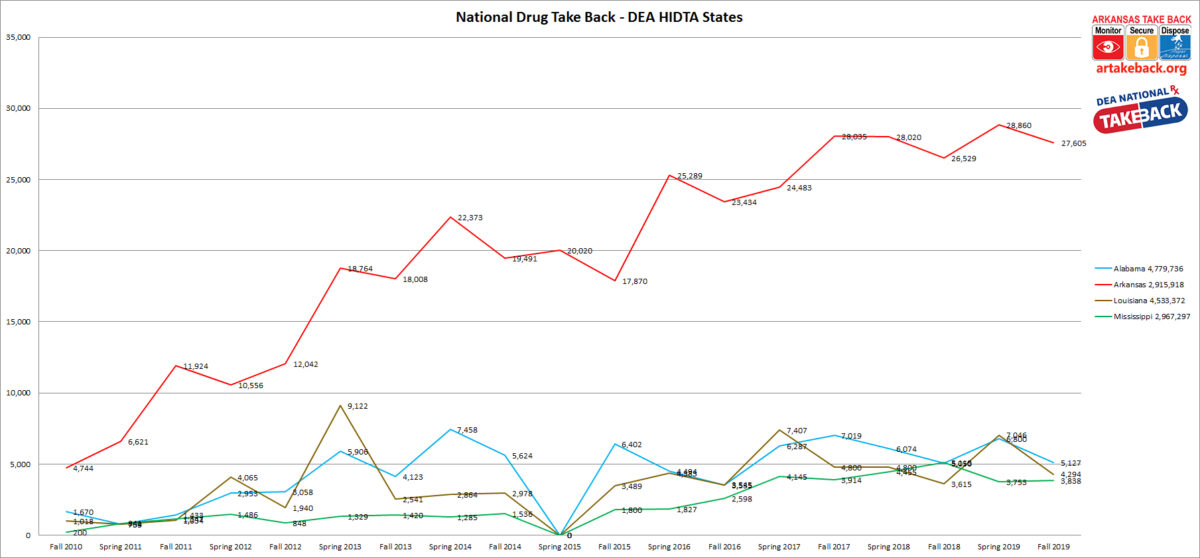
Arkansas continues to lead the four-state DEA region (Alabama, Arkansas, Louisiana, and Mississippi) accounting for 66% of all the medications collected. Arkansas also averages more participating law enforcement agencies than the other three states combined.
Arkansas Drug Take Back Day History
The Office of National Drug Control Policy (ONDCP), as part of its National Drug Control Strategy, called for an increase of prescription drug return and disposal programs as a means to curbing prescription drug abuse. Simultaneously, the Benton Police Department started a program called “Operation Medicine Cabinet” in the spring of 2010, after Russell Goodwin, owner of a local monument company and youth baseball coach, told then Benton Police Chief Kirk Lane that he was “tired of making headstones for children” he knew due to the abuse of prescription drugs. Benton officers gathered data that showed there was a problem with abuse and misuse of prescription drugs by youth, including information from the Saline County Coroner’s Office which showed that 30 people died in 2009 as a result of prescription drug abuse.
More than 146 pounds of prescription medications were collected at the first Operation Medicine Cabinet in Benton back in the spring of 2009, and the program and education to the public continued growth. State officials took notice and the program expanded. In 2010, a coalition led by then, State Drug Director Fran Flener, launched an on-going educational program to encourage everyone to “Monitor, Secure and Dispose” of their prescription medications. The also launched the website ardrugtakeback.org with an emphasis on educating and encouraging everyone to “Monitor, Secure, and Dispose” their prescription medications.
The U.S. Drug Enforcement Administration launched the National Prescription Drug Take Back Day on September 25, 2010 in response to an epidemic of controlled prescription drug (CPD) abuse in the United States.
Semi-annually a DEA Prescription Drug Take Back Day is held nationally. Arkansas supports this with core partners from the Arkansas Governor’s Office, Arkansas Attorney General’s office, Arkansas Department of Health, Arkansas Department of Human Services, Arkansas National Guard, Arkansas Rotary Clubs, Arkansas State Board of Pharmacy, Arkansas State Police, Office of Arkansas Drug Director along with more than 130 additional law enforcement and government agencies, numerous community organizations, businesses, media outlets, and public health providers. The Office of the Arkansas Drug Director works closely with the DEA in the coordination of this growing coalition, and in maintaining the Artakeback.org website.
One key to its success is the ability to have permanent collection boxes located at key locations throughout Arkansas communities. This allows the public to dispose of their unwanted medications throughout the year. Currently, Arkansas has more than 225 of permanent collection boxes, with at least one in every county in Arkansas. To find a collection box on ardrugtakeback.org click on the Collection Sites tab (or click this link: https://ardrugtakeback.org/take-back/collection-sites/ ) and type in a zip code, choose a distance and click the filter tab.
As part of the “Monitor, Secure, and Dispose” effort, the coalition organized Arkansas’s participation in the DEA’s National Prescription Take-Back Initiative, and take back events took place on September 25, 2010, April 30, 2011, October 29, 2011, April 28, 2012, September 29, 2012, April 27, 2013, October 26, 2013, April 26, 2014, and September 27, 2014. DEA announced the discontinuation of the national initiative in September 2014, but an Arkansas take back event under the leadership of partners within the state was held on April 25, 2015. DEA then reinstated the program nationally, and events since have been held on September 26, 2015, April 30, 2016, October 22, 2016, April 29, 2017, October 28, 2017, April 28, 2018, October 27, 2018, April 27, 2019, and October 26, 2019. [DISCLAIMER: **Collectively, there have been 18 total Arkansas Drug Take Back Day events, and 17 national events. Results from the State Take Back in spring 2015 were rolled into the total results for National Take Back 10 held September 26, 2015.]
Due to the commitment, dedication, and effort of the Arkansas Law Enforcement Community, its partners, and the multi-agency coalition, and due to excellent participation by Arkansans in all areas of the state, the take back events have been successful above and beyond all expectations.
The 18th Drug Take Back Day resulted in a total medications collection of 441.5 tons nationally and 13.8 tons in Arkansas. The grand total of all Drug Take Back Day events have resulted in 11,669.60 tons nationally and 187.227 tons in Arkansas.
STATISTICAL INFORMATION – National Comparison (Including all 18 events):
♦ Arkansas ranked #3 nationally in pounds collected per capita with 0.125 pounds per person. Maine ranked 1st with 0.308 pounds per person and Wisconsin ranked 2nd at 0.126 pounds per person.1
♦ Despite being thirty-third in population among all states, Arkansas ranked #13 in total weight1
♦ Arkansas ranked 9th in the amount of law enforcement agency participation with 192. Texas ranked 1st with 299 agencies. Washington D.C. ranked last with 1 agency. Nationally, 4,896 law enforcement agencies participated.2
♦ Arkansas ranked 13th in the number of collection sites with 183. Texas ranked 1st with 363 and North Dakota was last with 5.
♦ The four-state DEA region consisting of Alabama, Arkansas, Louisiana, and Mississippi pooled a total weight of 40,864 pounds for the 18th Drug Take Back Day and 569,680 pounds for all 18 Drug Take Back Day events. Arkansas, despite being the least populated state of the DEA region accounted for 66% of the total weight. Arkansas also averages more law enforcement participation than the other three states combined.
For Take Back 18, only:
♦ Arkansas ranked #13 nationally in weight collected (#1-#12: California, Texas, Wisconsin, New York, Illinois, Pennsylvania, Ohio, Missouri, Maine, Florida, Massachusetts, & Virginia)
♦ Ranked 4th per capita. Maine ranked #1, followed by Vermont, and Wisconsin, respectively.
♦ Ranked 9th in the number of Law Enforcement agencies participation.
♦ Ranks 13th in the number of registered collection sites.
1 Determined using 2017 census estimates. 2 Determined using data supplied by the National DEA.
STATISTICAL INFORMATION – Local Comparison:
Weight Collected Per Law Enforcement Agency (Take Back 18, only):
♦ Pulaski County Sheriff’s Office ranked #1 with 3,752 pounds collected (14% of the state’s total)
♦ Washington County Sheriff’s Office ranked #2 with 1,496 pounds collected (5.4% of the state’s total)
♦ Benton Police Department ranked #3 with 1,065 pounds collected (3.9% of the state’s total)
♦ Baxter County Sheriff’s Office ranked #4 with 1,019 pounds collected (3.7% of the state’s total)
♦ North Little Rock Police Department ranked #5 with 857 pounds collected (3.1% of the state’s total)